
The genus Streptococcus comprises more than 37 species and is classified as aerotolerant, fermentative, gram-positive cocci. They are usually catalase positive, non-sporing, and non-motile except Streptococcus sanguis, which shows twitching motility with polar fimbriae. According to Brown (1919), there are three types of Streptococci based on haemolytic reactionsobserved on bloodagar, i.e. alpha- haemolytic, beta-haemolytic and gamma-haemolytic Streptococci. Streptococcus pyogenes falls under the beta-haemolytic streptococci, which is also known as complete haemolysis. S. pyogenes is one of the most pathogenic among haemolytic Streptococci that are pathogenic to humans and falls into group A. Their cell division occurs in a single plane to form chains.

Taxonomy and Classification
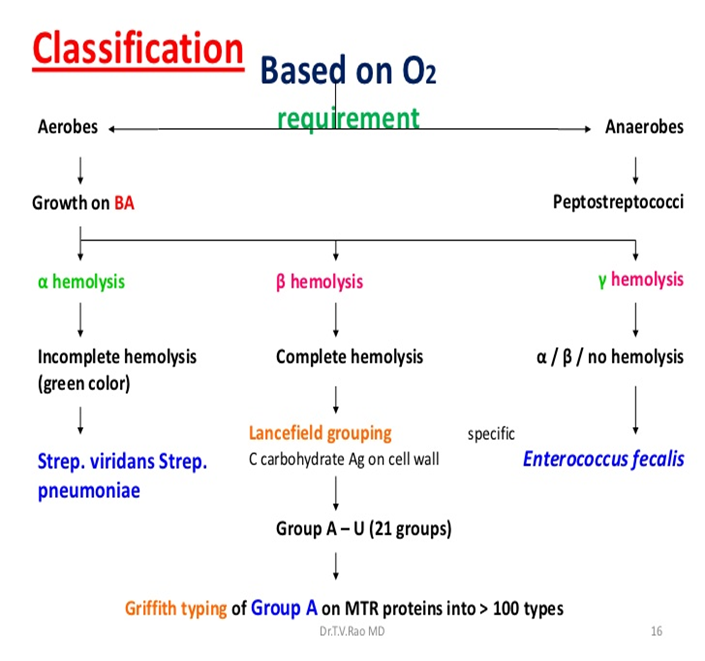
Fig 1: Classification of Streptococcus
Image source: https://www.onlinebiologynotes.com/classification-of-streptococcus/
Because Streptococci have an aerobic metabolism and are catalase positive, they were first divided into obligate anaerobes and facultative anaerobes. Then, when Brown introduced three terms, alpha, beta, and gamma, aerobic and facultative anaerobes were classified based on haemolytic reactions seen on blood agar plate and their antigen character. Beta-haemolysis is also known as complete haemolysis and is mostly pathogenic. Lancefield (1993) later classified most strains of beta haemolysis serologically into several broad groups A through H, K through V. Most pathogenic Streptococci pathogenic to humans are beta haemolytic and belong to the Group-A. S. pyogenes’ strains are subdivided into about 80 Griffith serotypes (type 1, type 2, type 3 etc.) according to their specific surface proteins i.e. M, T, and R. The production of surface protein M determines the pathogenicity of Streptococci.
Morphology and Microscopy
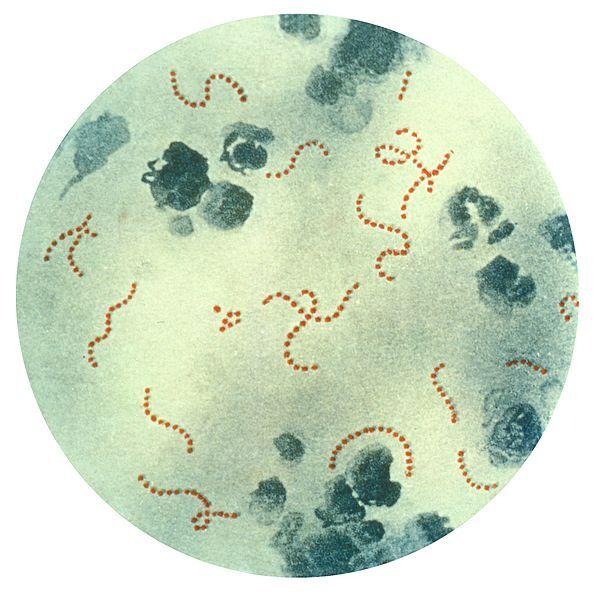
Fig 2: Chain-linked cocci of Streptococcus pyogenes
Image source: https://www.ncbi.nlm.nih.gov/books/NBK554528/figure/article-42960.image.f1/
S. pyogenes are spherical cocci that are about 0.5 to 1 μm in diameter which are arranged in pairs or in chains of up to 50 cells or more. These long chains are considered pathogenic strains whereas short-chain Streptococci are considered non-pathogenic strains. The length of the chain usually depends on cultural conditions such as temperature and agar media. They are non-sporing, capsulated or non-capsulated. Capsules of S. pyogenes or group-A are made up of hyaluronic acid.
Cultural and Growth Characteristics
- S. pyogenes are Gram-positive aerobes, facultative anaerobes which grow at a temperature of 37°C.
- Liquid media is best for the growth of larger chains than solid media.
- S. pyogenes grows well in blood agar and in media containing sugars (fermentable carbohydrates) and around 10% CO2 in the environment increases growth and haemolysis.
- They may appear gram negative if cultures are old or if the patient has been treated with antibiotics.
- Capsules of S. pyogenes are demonstrable only in young cultures during log phase of growth in liquid medium but with the onset of stationary phase, they are dissolved rapidly in the medium.
- On blood agar (BA), colonies are 0.5-1 mm after 24hrs, grayish white, transparent to translucent, with a large zone of beta haemolysis.
- Non capsulated strains produce matt (finely granular colonies) while capsulated strains produce glossy colonies.
- The yield of cells from broth cultures e.g., Todd- Todd- Hewitt broth is increased by the addition of a fermentable carbohydrate.
- On MacConkey agar (MA), they usually don’t grow but grow on gram positive selective media i.e. CAN (Columbia agar with colistin and nalidixic agar), PEA (Phenylethylalcohol agar).

Fig 3: Streptococcus pyogenes inoculated on trypticase soy agar containing 5% defibrinated sheep’s blood.
Image source: https://www.medlink.com/media/dlsc48
Biochemical and Identification
- Catalase negative
- Oxidase negative
- Ferment sugar to produce acid but no gas
- Urease negative
- Not soluble in 10% bile
- Non-motile
- Capsulated
- Usually, homofermentative (the predominant end product of sugar fermentation being lactic acid)
- S. pyogenes is the only species of beta-haemolytic streptococci that gives positive PYR (Pyrrolidonyl arylamidase) test.
Virulence Factors and Pathogenesis
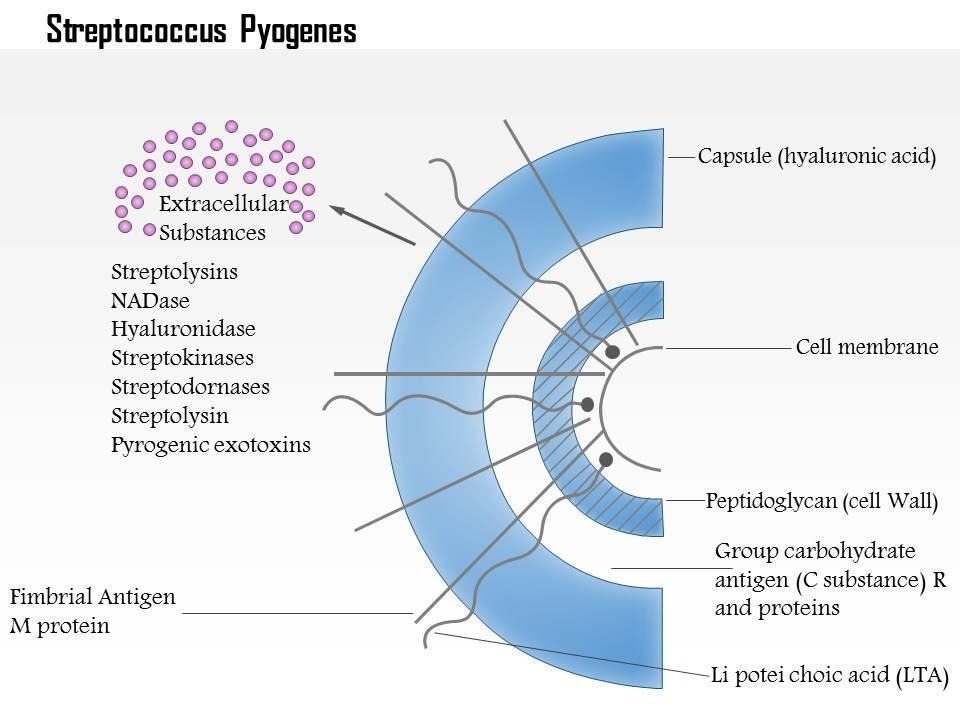
Fig 4: Group A Streptococcus pyogenes
Image source: https://www.slideteam.net/0614-streptococcus-pyogenes-medical-images-for-powerpoint.html
There are many virulence factors of group A streptococci which are described below:
- Capsule: Capsular hyaluronic acid is found in group A (S. pyogenes) and group C (S. equi but not S. equisimilis) streptococci during log phase of growth. But it is destroyed due to the production of hyaluronidase during the stationary phase. Therefore, the capsule is observable only in fresh cultures and capsulated strains form mucoid colonies on BA. Capsule production is encoded by HAS operon which contains at least 3 genes i.e. hasA, hasB and hasC.
- Group-specific polysachharide antigen: Normally, Streptococci contain specific types of polysachharide antigen in their cell wall on the basis of which they are classsified into different groups. Group A, Streptoccus pyogenes’ cell wall contains three layer which are an outer layer (fimbria containing protein), middle layer of group-specific carbohydrate (rhamnose-n-acetylglucosamine) and an inner layer of peptidoglycan (mucopeptide). The molecules of Group polysachharides are believed to have chemically similar structures with human tissues because of which S. pyogenes may become auto-reactive and lead to the pathogenesis of endocarditis, glomerulonephritis and so on.
- Type specific antigen: M protein, T and R proteins are included in type specific antigen. M proteins are mainly found in group A and also in S. agalactiae, S. dysgalactiae, S. sangius. They are distributed on the surface of the cell in association with fimbriae. Also, they may promote bacterial accumulation at the site of infection as a result of coaggregation between bacterial cells. T proteins are heat labile but resists proteolytic enzymes.
- Exotoxins: It contains various toxins such as: erthrogenic toxins, exotoxin A, exotoxin B and cardiohepatic toxin.
- Haemolysin S and O, also called streptolysins, are produced by S. pyogenes. It includes streptolysin O and streptolysin S. Streptolysin O is a protein and is responsible for beta haemolysin. Similarly, surface colony haemolysis is caused by an oxygen stable haemolysin streptolysin S.
Epidemiology and Transmission
S.pyogenes infection occurs worldwide; developing countries are at higher risk. However, since the 1980s even developed countries such as North America, Europe etc have reported increasing cases of S. pyogenes infection. The infection is more frequent to school-age children than in children less than 3 years old. The bacteria are transmitted through respiratory droplets and through direct contact.
Clinical Manifestations
There are two types of infection caused by S. pyogenes, they are: suppurative infections and non-suppurative complications.
- Suppurative infections: They are the primary infections. They cause pharyngitis (sore throat) and infections of respiratory tract which are classified by pain, redness and swelling of the posterior pharynx, accompanied by greyish white tonsillar exudate, fever etc. Although pharyngitis caused by S. pyogenes is normally self limiting, possible complications include infections of upper and lower respiratory tract for e.g. acute sinusitis, otitis media, cervical lymphadenitis and pneumonia.
When the infecting strain produces a pyrogenic or erythrogenic toxin, scarlet fever occurs as a complication of pharyngitis or other streptococcal infection, and the patient has no antitoxic immunity, usually a child. A red rash usually starts on the upper chest and spreads to other body parts. At the onset of disease, the tongue is covered by a thick white coat that is changed to a bright colour at the end of the week. Many forms of scarlet fever are life threatening.
Streptococcal impetigo is characterized by superficial skin lesions, usually less than 2.5 cm in diameter that resolve within 1-2 weeks of initial appearance. The lesions the develops from a papule to a small vesicle surrounded by a zone of erythema. While colonizing organisms lesions can arise and are introduced as broken skin via minor trauma or insect bites. Erysipeals is an acute spreading inflammation of skin, often on face. Necrotizing fasciitis refers to the invasive soft tissue infection originally called gangrene.
- Non-suppurative sequelae: The two important non-suppurative sequences are acute rheumatic fever and acute glomerulonephritis. Acute rheumatic fever may be followed by infection of any serotype of S. pyogenes but certain M proteins 5, 18 and 24 are more frequently associated. A protein called endostreptosin can be detected beneath the glomerular basement membrane during early stages of cutaneous streptococcal infection. The antigens react with antibodies produced by patients with glomerulonephritis.
Laboratory Diagnosis
Specimen: Lesion swab, pus swab or blood depending upon the nature of infection. Swabs are taken from the throat, vagina or lesion of patients.
Gram-staining: Gram positive spherical or oval cocci in chains or pairs
Culture: Blood agar is used as the medium. The specimen is inoculated in BA and is incubated at 37°C for 24hrs. Under anaerobic conditions or under 5-10% CO2, haemolysis is observed. Bacitracin is used for S.pyogenes as it is more sensitive to bacitracin than other streptococci and gives a zone of inhibition of diameter more than or equal to 11mm around a 6mm disc containing 0.04U of bacitracin.
Antigen detection tests: Rapid test kits of ELISA, and agglutination tests are very common these days to determine group A streptococcal antigen from throat swabs which are 75-80% sensitive.
Serological tests: Antibodies detection is commonly used for non suppurative complications diagnosis in comparison to suppurative diagnosis because most antibodies of toxins and enzymes of group A are produced late.
Treatments
Antibiotics such as Penicillin are used as group A beta-haemolytic streptococci are very sensitive to it. Another one is erythromycin or an oral cephalosporin is used in place of penicillin for those patients who are allergic to penicillin. Long term prophylactic antibiotic therapy is used to prevent recurrence of rheumatic fever.
Prevention and Control
- Direct contact with infected people should be maintained.
- Detection of cases and carriers and early microbial therapy can be included as control procedures.
Conclusion
In conclusion, S. pyogenes are gram positive streptococci, an important human pathogen which are responsible for causing various pathogenic infections worldwide. They holds major clinical impact because of its virulence, persistence and antibiotic resistance, mainly in school-age children.
References
Efstratiou A, Lamagni T. Epidemiology of Streptococcus pyogenes. 2022 Oct 30 [Updated 2022 Nov 7]. In: Ferretti JJ, Stevens DL, Fischetti VA, editors. Streptococcus pyogenes: Basic Biology to Clinical Manifestations [Internet]. 2nd edition. Oklahoma City (OK): University of Oklahoma Health Sciences Center; 2022 Oct 8. Chapter 19. Available from: https://www.ncbi.nlm.nih.gov/books/NBK587100/
Greenwood D, Black R C B and Peutherer J F 1997 Medical Microbiology, 15th Edn. Edinburgh : Churchill Livingstone.
Murray PR, Baron EJ, Pfaller MA, Tenover FC, Yolken RH (eds) 1999 Manual of Clinical Microbiology, 7th edn. Washington, DC : ASM Press.
Stevens DL 1992 Invasive grop A streptococcus infections. Clinical Infectious Diseases 14 : 2-11.